Anesthesia Side Effects
Research Spotlight

Meet Dr. Cecilia Canales, Anesthesiologist at UCLA Health
Anesthesiologists help minimize the pain and risks patients experience before, during, and after intensive medical procedures, such as surgery.
UCLA anesthesiologist and Simulation Center Medical Director, Cecilia Canales, MD, MPH, MS, feels grateful to do the work she does.
"I feel privileged to help patients when they are nervous or scared about surgery," she says. "I get to take care of them while they're undergoing intense and life-changing procedures."
Before Dr. Canales became an anesthesiologist, she'd been deeply connected to the UCLA community for decades—ever since her birth in fact, which happened at a UCLA hospital.
After completing her undergraduate education, she spent more than ten years gaining experience before going to medical school. She worked at UCLA conducting anesthesiology research and expanding Simulation Center training into various Health Sciences schools and residency programs.
"I knew nothing about anesthesia, and I knew nothing about simulation, but I found myself working all the time because everything truly interested me."
Her fascination with anesthesiology grew stronger throughout medical school. She loved doing research and clinical rotations in anesthesiology. She loved working with anesthesiologists. She had no doubts about what specialty she wanted to pursue.
Today, she remains as confident as ever in her choice.
"I love my job," says Dr. Canales. "I help people feel calm during some of the most anxious moments in their lives."
What Is Anesthesia? How Does It Work?
Anesthesia is a medical practice that incorporates pathophysiology and pharmacology. It minimizes the pain patients experience during intensive medical procedures, such as surgery.
There are multiple anesthesia types and administration methods. Anesthesiologists meticulously select anesthesia portfolios based on a patient's procedure and other individual factors.
"As an anesthesiologist, it's my job to keep patients safe and comfortable during a procedure that could otherwise be painful and traumatic," Dr. Canales explains.
On a pharmacological level, anesthesia works by stopping nerves from sending pain signals to the brain.
Speaking more generally, anesthesia can work as well as it does in a variety of different scenarios thanks to an anesthesiologist's planning, administration, and tireless monitoring and recalibration.
"During a procedure, I'm constantly tracking the patient's heart rate, blood pressure, blood loss, and other factors. I listen to the conversations in the room. I pay attention to everything that's going on and adjust as needed," Dr. Canales says.
Anesthesiologists work meticulously and constantly to keep anesthesia working for their patients. That's why a common misconception about the nature of anesthesiologists' work can be hurtful to those in the field.
Misconception: When anesthesiologists aren't actively administering anesthesia, they're doing absolutely nothing. It's easy work.
"Even when everything's quiet, I am doing so many different things."
Another UCLA anesthesiologist, Dr. Jason Lee, echoed Dr. Canales's sentiments. He says anesthesiologists function like lighthouses for their care teams. During procedures, they're constantly scanning the landscape for potential issues. If they detect something concerning, they alert the team and guide them toward a more favorable course.
Types of Anesthesia
Common types of anesthesia include:
Sedation / Twilight Anesthesia
Sometimes referred to as 'monitored anesthesia care' or 'sedation,' twilight anesthesia produces heavy drowsiness and relaxation but not full unconsciousness.
Twilight Anesthesia Side Effects
General Anesthesia
General anesthesia is induced by various anesthetic agents and medications. It puts patients in a state of full unconsciousness and affects the entire body.
General Anesthesia Side Effects
Regional Anesthesia
Regional anesthesia makes the specific region of a patient's body insensitive to pain prior to undergoing a localized procedure or surgery. Common examples of regional anesthesia include spinal and epidural anesthesia.
Regional Anesthesia Side Effects
Local Anesthesia
Local anesthesia, often induced via medications such as lidocaine, numbs a small area of the patient's body for minor and highly localized procedures. It significantly reduces but may not fully block all pain.
Common examples of local anesthesia include oral numbing for dental procedures or targeted numbing for wounds that require stitches.
General Anesthesia vs Sedation - What’s the Difference?
General anesthesia and sedation both reduce the sensations of pain patients experience. They differ primarily in terms of the level of unconsciousness they produce.
Under sedation, a patient remains conscious.
"Under moderate sedation, a patient is awake, but relaxed and drowsy," explains Dr. Canales. "They maintain awareness and can even talk throughout the procedure."
Even under deep sedation, when rousing a patient would take significant stimulus or pain, they're still just nearly unconscious—not fully.
Under anesthesia, a patient goes unconscious.
"In general anesthesia, we induce complete unconsciousness. That typically requires airway support. We help the patient breathe using tubes or assistive devices."
Anesthesiologists closely monitor the unconscious patient, adjusting medications, giving oxygen, and making other modifications to protect and support them.
Local Anesthesia vs Regional Anesthesia - What’s the Difference?
Local anesthesia and regional anesthesia both target specific areas of a patient's body that need to be insensitive to pain for a procedure.
These two anesthesia types affect areas of different sizes and block sensations of pain to different degrees.
Local anesthesia makes one small area of a patient's body numb to most sensations of pain. Common examples of local anesthesia include oral numbing for dental procedures or targeted numbing for wounds that require stitches.
"If a patient needs stitches, their physician might apply numbing medication around the skin, localized to the area they'll be working on," Dr. Canales explains.
Regional anesthesia makes entire sections of a patient's body, such as entire nerves or limbs, insensitive to pain. For example, an epidural provided for a cesarean section (C-section) childbirth procedure will make the patient insensitive to pain, but only from the waist down.
How Long Does Anesthesia Last?
Anesthesiologists determine how long anesthesia lasts by modifying their administration methods and dosages on a case-by-case basis.
The duration depends on the length of the procedure itself, the anesthesia type, and other individual factors. In general, anesthesia can last anywhere from hours to days.
"Anesthesia can last and indefinitely," Dr. Canales explains. "I've done surgeries that last more than 24 hours."
Returning to the example of an epidural provided for a cesarean section (C-section) childbirth procedure, Dr. Canales explains that a patient may need to be in labor for multiple days.
"I can make their epidural last for days by using a pump that has medication constantly being infused at a rate that we predetermine based on the patient's height, weight, medication and desired effect."

What Are the Side Effects of Anesthesia?
All types of anesthesia can and do produce side effects.
"In anesthesia, we induce unconsciousness," says Dr. Canales. "That comes with expected side effects related to how the medicines work."
Many anesthesia side effects are expected and easily resolved and managed. However, anesthesia itself, much like the procedures it enables, can lead to rare but serious side effects.
"I always tell my patients safety first and comfort second," says Dr. Canales. "Due to the nature of the procedures, or the patient’s comorbidities, I can't necessarily guarantee both."
Anesthesiologists might not be able to guarantee their patients' safety and comfort, but they work extremely hard to eliminate or significantly reduce as many risks as they can.
Prior to a procedure, anesthesiologists consult with other members of a patient's care team to collect their medical histories and all relevant details about lifestyle, pre-existing conditions, medications, and other individual factors.
General Anesthesia Side Effects
Short-Term Side Effects of General Anesthesia
Changes in blood pressure.
Patients under general anesthesia often experience changes in blood pressure. Anesthesiologists expect this and prepare accordingly.
"This side effect is part of the reason we constantly monitor blood pressure during the procedure, and we may even assist with managing it if needed."
Post-operative nausea and vomiting.
Many people, even individuals who avoid lifestyle risks such as smoking cigarettes, experience nausea and vomiting from anesthesia. Furthermore, some medications administered to control post-operative pain, such as opioids, can cause nausea.
This side effect may be eliminated or reduced by providing additional anti-nausea medications.
Sore throat.
A sore throat is a normal and expected side effect of the breathing support aspect of anesthesia.
"The breathing tubes we put in to help patients breathe can create some discomfort and soreness in the throat and mouth," Dr. Canales explains.
This side effect applies to any procedure requiring general anesthesia, even procedures taking place far from a patient’s throat.
Dental damage.
Dental damage, like throat soreness, is another side effect of general anesthesia stemming specifically from breathing tubes.
"When we put in a breathing tube, there could be dental damage, especially if a patient has chipped or loose teeth. We try to prevent that from happening, obviously, but it is a possibility, so it's included on the patient consent form."
Cold chills and low body temperature.
Anesthesia itself takes away the body's natural ability to regulate temperature. The medications that induce anesthesia are vasodilators, or blood-vessel dilators. They cause blood vessels to widen and blood flow and speed to increase, which in turn allows more heat to escape the body.
Muscle aches and shivering.
Anesthesiologists sometimes give patients muscle relaxants, which can cause shivering, also called vesiculation, as a side effect. The shivering, in turn, can cause muscle aches.
More broadly, patients may experience muscle aches from not moving for prolonged periods of time.
Long-Term Sides Effects of General Anesthesia
Postoperative cognitive changes.
Some patients experience cognitive changes, including dysfunction, after surgery.
Older individuals and those with pre-existing cognitive impairments face a greater risk of experiencing cognitive changes.
While this is a known side effect of receiving anesthesia, there's some debate across Dr. Canales's field around whether there's a direct causal relationship between surgery, anesthesia and cognitive change.
"There's a lot of research being done on the mechanisms and trying to determine what actually causes this," she explains. "Some believe it's a neuroinflammatory process from the surgery itself and has nothing to do with anesthesia, but surgery almost never happens without anesthesia so it's hard to isolate the direct causes of some side effects."
Malignant hyperthermia.
Malignant hyperthermia is a rare pharmacogenetic disorder linked to adverse hypermetabolic reactions to some anesthetic agents. The metabolic response can lead to a dangerous increase in the patient's body temperature.
"The body becomes very, very hot," says Dr. Canales. "This ultimately leads to muscle breakdown, essentially. It can affect the kidneys, blood, and everything else."
Malignant hyperthermia is a very rare inherited disorder, but it can lead to life-threatening consequences when an affected patient goes under general anesthesia.
Patients with family histories of malignant hyperthermia may be tested for the disorder via muscle biopsy, however the procedure is expensive and not 100% accurate.
Twilight Anesthesia / Sedation Side Effects
Short-Term Sides Effects of Twilight Anesthesia
Changes in blood pressure.
Patients under twilight anesthesia may experience changes in blood pressure.
Allergic reactions, such as itching or burning sensations.
Patients under sedation might experience unexpected allergic reactions to anything they have contact with during the procedure.
"I always tell patients that they can be allergic to anything in the room, including any of the medications we're going to give them.”
Allergic reactions tend to be mild, including itchiness or burning sensations localized to injection sites.
Drowsiness and grogginess.
Drowsiness and grogginess are natural and expected side effects of being sedated. Patients should expect to feel drowsy and plan accordingly.
Dr. Canales advises them to plan to avoid driving and making important life decisions.
"These medications interact with the brain," she says. "They will make patients drowsy and unreliable, at least for a few hours."
Nausea, dizziness, and forgetfulness.
Anesthetic medications can interact with the brain's memory centers. Patients may experience nausea, dizziness, and forgetfulness.
Additionally, the blood pressure changes that often happen during twilight anesthesia may also contribute to sensations of dizziness and lightheadedness.
Respiratory depression.
Respiratory depression describes a state where a patient's breathing slows to the extent that they're unable to intake adequate amounts of oxygen.
Patients with pre-existing respiratory concerns, such as asthma and obstructive sleep apnea, run a higher risk of experiencing respiratory depression.
Fortunately, anesthesiologists closely monitor this potentially problematic anesthesia side effect.
Respiratory depression may become bad enough that a patient under twilight anesthesia cannot protect their own airways. In these cases, an anesthesiologist may convert them to general anesthesia to better support their breathing.
"We can completely take over respiration for the patient by converting them from twilight anesthesia to general anesthesia and putting in breathing tubes or using other assistive devices."
Long-Term Sides Effects of Twilight Anesthesia
In general, twilight anesthesia lasts for only a short duration. Patients typically feel like their normal selves not long after the procedure and experience few, if any, long-term side effects.
Regional Anesthesia Side Effects
Short-Term Sides Effects of Regional Anesthesia
Blood pressure changes.
Patients under regional anesthesia may experience changes in blood pressure.
Headaches.
Post-dural puncture headaches (PDPH) are among the most common side effects of regional anesthesia targeting the spinal area, especially with epidural anesthesia.
"It's called an epidural because we put medication right into a membrane called the dura. Nerves up and down the spine absorb the numbing medication from the epidural space, and that's what helps mitigate pain," Dr. Canales says
If an anesthesiologist goes too far into the dura membrane when administering the epidural, a post-dural puncture headache can occur.
Post-dural puncture headaches usually resolve relatively quickly. Symptoms may be mitigated by simple interventions such as acetaminophen, hydration, and even caffeine.
Long-Term Sides Effects of Regional Anesthesia
Paralysis, infection, and blood loss.
Dr. Canales's hears from many patients concerned about their risk of developing paralysis.
She tells them that while developing paralysis from regional anesthesia is extremely unlikely, there's always a risk of complications when undergoing any procedure. Furthermore, complications may be extremely hard to forecast.
"We do many safety tests to minimize the risk of serious complications," she says.
"However, whenever we introduce a needle, there are numerous potential risks including the risk of infection, blood loss, and even nerve damage due to accidental entry into a vein or artery."
Hematoma.
Hematoma refers to a rare local anesthesia side effect.
Hematomas develop when blood collects outside veins or blood vessels and cannot drain properly. They can form anywhere in the body—even in tissues and important organs, such as the brain.
After regional anesthesia targeting the spinal area, a hematoma can develop and compress a patient's spinal cord.
Before, during, and after procedures, anesthesiologists do everything possible to gauge and mitigate a patient's risk of developing a hematoma.
"It's a rare risk, and it's why we always check platelets, blood counts, and medications that may cause bleeding before a patient undergoes a procedure," Dr. Canales says.
Local Anesthesia Side Effects
Compared to other types of anesthesia, local anesthesia is linked with the fewest and the least severe side effects.
Patients receiving local anesthesia will likely experience minor unpleasant sensations, including numbness, tingling, swelling, and pain. These sensations are simply caused by the local anesthetic having its intended effect and are not considered side effects.
In some very rare cases, local anesthesia may lead to nerve damage and allergic reactions that have significant, long-term consequences.
Common Misconceptions and Frequently Asked Questions About Anesthesia
Does Anesthesia Cause Constipation?
Anesthetic medications that induce anesthesia do not directly cause constipation. However, many people do experience constipation after undergoing anesthesia.
"We give pain medications during and after procedures that make it feasible for surgeons to be able to do something that is truly painful. The downside is that those medications can cause constipation by slowing down the transit of food."
Furthermore, the reduced mobility and fasting required for intense procedures can often lead to constipation.
Does Anesthesia Cause Hair Loss?
As with constipation, there is no evidence that anesthetic medications directly cause hair loss.
Dr. Canales says nutrient deficiencies and some medications, including antibiotics or steroids, can contribute to hair thinning, but there is no pharmacological link between the anesthetics and hair loss.
Is Anesthesia the Same as Sleep?
Going under anesthesia is not the same thing as going to sleep. Sleep produces an altered state of consciousness. Anesthesia produces full unconsciousness.
"I never tell my patients that they're going to sleep because it's not sleep," explains Dr. Canales. "Sleep has very specific brainwaves, and when we induce general anesthesia, they're different brainwaves."
Can a Patient Wake Up During Anesthesia?
Anesthesiologists closely monitor patients under anesthesia and continually adjust medications to maintain the desired level of unconsciousness for the desired length of time.
It's extremely unlikely that a patient would wake up before the intended time.
Dr. Canales's patients sometimes tell her they think they woke up in the middle of anesthesia. She guesses they're remembering being woken up from anesthesia after their procedure—not waking up during it.
Is Anesthesia Dangerous?
Anesthesiologists work extremely hard and undergo years of training to manage the natural risks of anesthesia and make it as safe and comfortable as possible for patients before, during, and after procedures.
Unmonitored anesthesia would technically be dangerous, but it’s extremely unlikely any patient would ever find themselves in such a circumstance thanks to anesthesiologists.
Anesthesia Research at UCLA
In addition to caring for patients as an anesthesiologist, Dr. Canales also conducts anesthesia research.
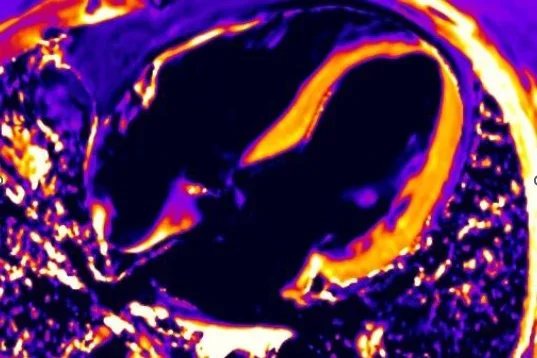
Specifically, she studies cognitive changes after surgery and frailty. She has used point-of-care ultrasound to measure patient frailty before surgery, which has been linked to postoperative neurocognitive disorders, such as delirium and cognitive dysfunction.
Dr. Canales has been examining frailty and post-operative cognition since she first learned they were correlated during residency.
"I learned frail patients had worse mortality rates and a higher risk of developing delirium than other patients," Dr. Canales says. "This surprised me because we do not get instruction on frailty as part of our formal anesthesia training."
She imagined there had to be a way to identify frail patients at risk for experiencing cognitive issues. Brainstorming solutions with Dr. Singh, her mentor, led her to point-of-care ultrasound and the research she's engaged with to this day.
"I use point-of-care ultrasound to measure muscle mass and identify frail patients."
Anesthesiologists need all of the information they can possibly have about a patient to create optimal anesthesia plans. Unfortunately, they sometimes have barely any information at all.
"When a trauma patient comes in for an emergency procedure, we often don't have their histories, charts, medication lists, etc.," says Dr. Canales.
It's even more complicated when a patient is unable to answer or react to questions—when they arrive at the hospital unconscious.
In these and similar cases, point-of-care ultrasound provides Dr. Canales and other anesthesiologists with a method of quickly collecting accurate information about a patient to better inform their anesthesia approach.
"It's about making small adjustments for each patient," says Dr. Canales. "It's about doing what we can to ensure surgery can proceed in the most safe and efficient manner possible."
That's the core value at the heart of Dr. Canales's research—making anesthesia as safe and effective as possible, not just for older adults but for all groups underrepresented in the current practices. (She earned a place in the National Academy of Medicine Scholars in Diagnostic Excellence program for her project proposal, “Advancing Language Equity in Diagnosing Perioperative Neurocognitive Disorders.”)
When Dr. Canales first began researching frailty and postoperative outcomes, her literature reviews made her aware of another patient population facing inequitable postsurgical outcomes.
"As I was reading the literature, I noticed that nearly every study done in the United States excluded patients who don't speak English."
Dr. Canales's family immigrated from Mexico. She speaks Spanish and can effectively communicate with the numerous Spanish-speaking patients she sees. She found it unacceptable that patients elsewhere might face suboptimal outcomes just because they don't speak English.
"That's why we all need to go back and take another look at everything," she says. "We need to find these gaps and inequities and adjust what we do to make things better for all the diverse groups of patients we care for, regardless of what language they speak."